Polymicrobial infection in immunocompromised host - How to manage?
|
|
Polymicrobial infection in immunocompromised host - How to manage?
22/06/2024
22/06/2024
https://www.pediatriconcall.com/Journal/images/journal_cover.jpg
Meenakshi Dey1, Suhani Jain2, Ira Shah3.
1Department of Pediatric Infectious Diseases, B J Wadia Hospital for Children, Mumbai, Maharashtra, India,
2Grant Government Medical College, Sir JJ Group of Hospitals, Mumbai, India,
3Consultant in Pediatric Infectious Diseases, Levioza Health Care, Mumbai, India.
ADDRESS FOR CORRESPONDENCE
Suhani Jain, Flat number 402, Ramdeo Arise, Behind Hotel Airport Centre Pt, Wardha Road, Nagpur-440025.
Email: suhani2208@gmail.com
Immunocompromised infants, STAT1 mutation, Polymicrobial infection
|
Clinical Problem
A 2 year 9 month old male suffering from STAT1 gain of function mutation on whole exome sequencing diagnosed at the age of 6 months in view of recurrent pneumonia presented to us with fever and cough for 15 days. There was no exposure to a patient with tuberculosis. The child was on baricitinib for past 2 years. He was also on fluconazole prophylaxis for initial 6 months and then oral voriconazole for 6 months for fungal prophylaxis but was off antifungal for the past 6 months. On presentation, the child weighed 9.6 kg [weight for age <3rd centile as per Indian Academy of Pediatrics (IAP) growth chart], height was 88 cm (length for age 3rd to 50th centile as per IAP growth chart), heart rate was 130/min, respiratory rate was 42/min with mild respiratory distress and subcostal retractions. Oxygen saturation was 88 % on room air. Other general examination was normal. On respiratory system examination, there were bilateral crepts in mammary and axillary regions on auscultation. Other systemic examination was normal. Child was started on supportive treatment with intravenous fluids, oxygen by nasal prongs, broad spectrum antibiotics (injectable meropenem at 20 mg/kg/dose 8 hourly and vancomycin at 15 mg/kg/dose 8 hourly) with antifungal (Injectable fluconazole at 12 mg/kg/dose once a day) and baricitinib was stopped. Investigations are depicted in Table 1. Chest X-ray had right lower zone inhomogenous opacification with cavity with infiltrates in bilateral lungs as shown in Figure 1. HRCT chest showed necrotising pneumonia with large irregular air filled cavitatory lesion and multiple necrotic foci in the right lower lobe along, similar area of consolidation and necrosis in the right middle lobe, nodular infiltrates in both lungs with subsegmental areas of consolidation in the left lower lobe. Gastric lavage (GL) Xpert Mtb/Rif assay detected mycobacterium tuberculosis with no rifampicin resistance. Antituberculous therapy (ATT) consisting of isoniazid (H) (8 mg/kg/day), rifampicin (R) (20 mg/kg/day), pyrazinamide (Z) (35 mg/kg/day), ethambutol (E) (25 mg/kg/day) was started. Bronchoalveolar lavage (BAL) fungal culture grew Candida tropicalis resistant to fluconazole and voriconazole and sensitive to amphotericin B, caspofungin and micafungin. Hence Liposomal Amphotericin B was started at 3 mg/kg/day and fluconazole was stopped. Blood culture did not grow any organism. Ultrasound abdomen was normal. BAL and whole blood cytomegalovirus (CMV) PCR was positive hence oral valganciclovir (520 mg/sqm/day) was added. BAL multiplex PCR showed adenovirus for which the child was given intravenous immunoglobulin (IVIG) at dose of 400 mg/kg. Child became afebrile for 48 hours, but again started developing new onset fever spikes with aggravation of cough. Throat swab showed presence of influenza A and H3N2 on PCR for which oseltamivir (3mg/kg/dose 12 hourly for 10 days) was added. Child became afebrile after 72 hours and oxygen saturation was maintained on room air. Blood CMV PCR was negative after 2 weeks of therapy. After 14 days of Inj amphotericin B, posaconazole was added at dose of 6 mg/kg/dose 8 hourly. Child was shifted to Rifampicin devoid regimen of ATT and ofloxacin was added and HZE was continued. Amphotericin B was stopped after 21 days and posaconazole trough levels were sent. Posaconazole trough levels were <0.1, hence dose was increased by 25% and advised to repeat trough levels after 1 week. Repeat Chest Xray after 3 weeks showed some improvement as shown in Figure 2. He was discharged after 40 days of hospitalization on H, Z, E, ofloxacin, valganciclovir, posaconazole, pyridoxine.
Figure 1. Chest X-ray showing lower zone inhomogenous opacification with cavity with infiltrates in bilateral lungs.
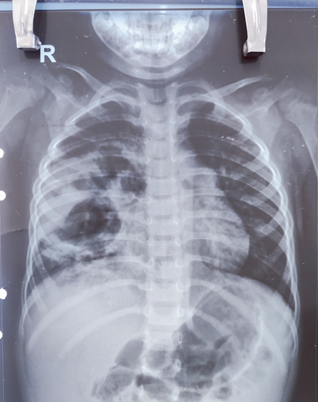
Figure 2. repeat CXR after 1 month showing improvement.
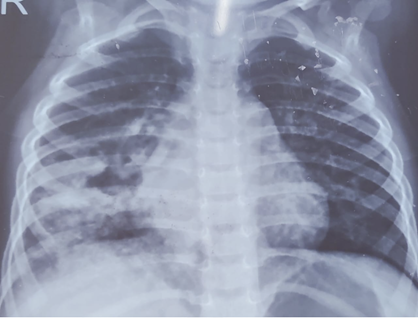
Table 1. Serial laboratory parameters of the patient.
| Laboratory parameter |
Day of presentation |
Day 5 |
Day 9 |
Day 11 |
Day 16 |
Day 18 |
Day 21 |
| Hemoglobin (g/dL) |
9.9 |
|
|
|
|
|
|
| Total leucocyte count (cells/cumm) |
11,480 |
| Absolute neutrophil count (cells/cumm) |
9115 |
| Absolute lymphocyte count (per cu.mm) |
1572 |
| Platelet count (cells/cumm) |
3,06,000 |
| C-reactive protein (g/L) |
166 |
87 |
|
|
5 |
|
|
| Blood culture |
Negative |
|
|
Negative |
|
|
|
| Xpert Mtb/Rif (Gastric lavage) |
M.tb detected very low, rif resistance not detected |
|
|
|
|
|
|
| BAL Multiplex PCR |
|
|
Adenovirus detected |
|
|
|
|
| Whole blood CMV Quantitative PCR |
|
|
8564 copies/ml
Log10 value 3.93 |
|
|
|
Below limit of detection |
| BAL Quantitative CMV PCR |
|
|
103695 copies/ml
Log10 value 5.01 |
|
|
|
|
| BAL gram stain |
|
|
Few pus cells |
|
|
|
|
| BAL KOH mount |
|
|
Negative |
|
|
|
|
| BAL bacterial culture |
|
|
Streptococcus sanguinis |
|
|
|
|
| BAL fungal culture |
|
|
Candida tropicalis (colony count of <103 cfu/ml) |
|
|
|
|
| Throat swab for influenza |
|
|
|
|
|
Influenza A: detected
H3N2: detected
H1N1: not detected
Influenza B: not detected
|
|
|
| |
How should patients with polymicrobial infections in immunocompromised patients be treated?
|
|
|
Discussion
Signal transducer and activator of transcription 1, commonly known as STAT1, holds significant importance within the STAT family. It plays a crucial role in governing various cellular processes such as growth, differentiation, proliferation, metabolism and programmed cell death by engaging the JAK-STAT pathway.1,2,3 initial reports documented the occurrence of germline STAT1 Loss of Function (LOF) mutations associated with Mendelian susceptibility to mycobacterial disease (MSMD) and STAT1 Gain of Function (GOF) mutations linked to chronic mucocutaneous candidiasis (CMC). Subsequent research has affirmed that both STAT1-GOF and LOF germline mutations lead to immune deficiency and immune dysregulation, manifesting a broad range of clinical manifestations. The patient under our consideration was found to have a STAT1 GOF mutation.4,5,6
STAT1 Gain of Function (GOF) mutations can lead to a diverse spectrum of manifestations, encompassing mucocutaneous fungal infections resulting from Candida albicans, along with ear, nose and throat (ENT) infections, as well as lower respiratory infections provoked by Streptococcus species, Staphylococcus aureus and Pseudomonas aeruginosa.7 Our patient had a prior medical history of recurring oral candidiasis, which required voriconazole prophylaxis. He was also on baricitinib (JAK inhibitor). Inspite of this, he presented with a wide range of infections which posed a significant management challenge. As per literature, management of patients with severe infectious and autoimmune symptoms stemming from STAT1-GOF mutations primarily involve hematopoietic stem cell transplantation and/or the administration of oral JAK inhibitors.8
We adopted targeted treatment strategy to address the various infections. Extensive screening was conducted to identify the specific infections, leading to a treatment plan that encompassed the use of ATT with H, Z, E ofloxacin for TB, Liposomal Amphotericin B and posaconazole to combat pulmonary candidiasis, oral valganciclovir for CMV, intravenous immunoglobulin (IVIG) for adenovirus and oseltamivir to manage influenza A and H3N2. We preferred to give IVIG instead of cidofovir for adenovirus infection inspite of it being recognised for use in immunocompromised state because of its drug interaction with amphotericin B leading to side effects like nephrotoxicity and ototoxicity.9,10
Candida spp are considered a part of the normal microflora of the skin, oral cavity, gastrointestinal mucosa, respiratory tract and genitourinary tract.11 It is not possible to distinguish between commensal, colonizer and true candida infection. In immunocompromised patients, candida might be isolated from respiratory specimens such as sputum and BAL, but it should be interpreted with caution. The true incidence of Candida spp pneumonia ranges from 0.23% to 0.4%.12,13 The diagnosis of Candida spp pneumonia is difficult due to the nonspecific clinical and radiological features and the lack of specific biomarkers which necessitates the histopathological demonstration of the organism for confirmation of diagnosis. Colonization of the respiratory epithelium by Candida species is a prerequisite of invasive infections. The predominant risk factors for invasive candidiasis are immunocompromised host, repeated use of broad-spectrum antibiotics, severe neutropenia, chemotherapy-induced mucositis and prolonged hospital stay.14,15
The treatment of candida in BAL fluid is largely controversial. In our case we decide to treat the candida tropicalis isolate, as child was suffering from STAT1 mutation which made him prone to mucocutaneous candidiasis. In our case, Candida drug susceptibility testing was done by vitek automated system, which showed resistance to fluconazole and voriconazole. Posaconazole MIC was 0.50 mcg/ml, however guidelines are not defined for interpretation. We started posaconazole at 18 mg/kg/day in 3 divided doses as oral suspension.16 Since posaconazole interacts with rifampicin17, the latter was stopped and ATT was shifted to HZE and ofloxacin. Oral valganciclovir for CMV and oseltamivir to manage influenza A is also indicated for use in immunocompromised children.18,19 Hence while treating polymicrobial infection, it’s important to keep drug interactions in mind. On follow up, posaconazole trough levels were obtained which were <0.1 which is below the recommended range of 1 mcg/ml for treatment hence dose was increased and child was asked to follow up after 1 week with repeat levels.16
|
| |
| Compliance with ethical standards |
|
Funding: None
|
|
|
Conflict of Interest: None
|
- Yang Q, Yu C, Wu Y, Cao K, Li X, Cao W, et al. Unusual Talaromyces marneffei and Pneumocystis jirovecii coinfection in a child with a STAT1 mutation: A case report and literature review. Front Immunol. 2023;14:1103184. doi: 10.3389/fimmu.2023.1103184. [CrossRef] [PubMed] [PMC free article]
- Stark GR, Darnell JE. The JAK-STAT pathway at twenty. Immunity. 2012;36:503-514. doi: 10.1016/j.immuni.2012.03.013 [CrossRef] [PubMed] [PMC free article]
- Ivashkiv LB. IFNγ: signalling, epigenetics and roles in immunity, metabolism, disease and cancer immunotherapy. Nat Rev Immunol. 2018;18:545-558. doi: 10.1038/s41577-018-0029-z [CrossRef] [PubMed] [PMC free article]
- Dupuis S, Dargemont C, Fieschi C, Thomassin N, Rosenzweig S, Harris J, et al. Impairment of mycobacterial but not viral immunity by a germline human STAT1 mutation. Science. (2001) 293:300-3. doi: 10.1126/science.1061154 [CrossRef] [PubMed]
- Liu L, Okada S, Kong XF, Kreins AY, Cypowyj S, Abhyankar A, et al. Gain-of-function human STAT1 mutations impair IL-17 immunity and underlie chronic mucocutaneous candidiasis. J Exp Med. (2011) 208:1635-48. doi: 10.1084/jem.20110958 [CrossRef] [PubMed] [PMC free article]
- van de Veerdonk FL, Plantinga TS, Hoischen A, Smeekens SP, Joosten LAB, Gilissen C, et al. STAT1 mutations in autosomal dominant chronic mucocutaneous candidiasis. N Engl J Med. (2011) 365:54-61. doi: 10.1056/NEJMoa1100102 [CrossRef] [PubMed]
- Zhang W, Chen X, Gao G, Xing S, Zhou L, Tang X, et al. Clinical Relevance of Gain- and Loss-of-Function Germline Mutations in STAT1: A Systematic Review. Frontiers in Immunology [Internet]. 2021;12. [CrossRef] [PubMed] [PMC free article]
- Okada S, Asano T, Moriya K, Boisson-Dupuis S, Kobayashi M, Casanova JL, et al. Human STAT1 Gain-of-Function Heterozygous Mutations: Chronic Mucocutaneous Candidiasis and Type I Interferonopathy. J Clin Immunol. 2020/08/27 ed. 2020 Nov;40(8):1065-81. [CrossRef] [PubMed] [PMC free article]
- Wade RL, Chaudhari P, Natoli JL, Taylor RJ, Nathanson BH, Horn D. Comparison of adverse events and hospital length of stay associated with various amphotericin B formulations: sequential conventional amphotericin b/lipid versus lipid-only therapy for the treatment of invasive fungal infections in hospitalized patients. P T. 2013 May;38(5):278-87.
- Alcamo AM, Wolf MS, Alessi LJ, Chong HJ, Green M, Williams JV, et al. Successful Use of Cidofovir in an Immunocompetent Child With Severe Adenoviral Sepsis. Pediatrics. 2020;145:e20191632. [CrossRef] [PubMed] [PMC free article]
- Kumamoto CA, Vinces MD. Alternative candida lifestyles: growth on surfaces. Annu Rev Microbiol. 2005;59:113-33. [CrossRef] [PubMed]
- Masur H, Rosen PP, Armstrong D. Pulmonary disease caused by Candida species. Am J Med. 1977 Dec;63(6):914-25. [CrossRef] [PubMed]
- Haron E et al. Primary Candida pneumonia. Experience at a large cancer center and review of the literature. Medicine. 1993;72:137-42 [CrossRef]
- Petty LA et al. Candida dubliniensis pneumonia: a case report and review of literature. Mycopathologia. 2016;181: 765-8 [CrossRef] [PubMed]
- Tan M, Wang J, Hu P, Wang B, Xu W, Chen J. Severe pneumonia due to infection with Candida krusei in a case of suspected Middle East respiratory syndrome: a case report and literature review. Exp Ther Med. 2016;12:4085-4088. [CrossRef] [PubMed] [PMC free article]
- Bernardo VA, Cross SJ, Crews KR, Flynn PM, Hoffman JM, Knapp KM, et al. Posaconazole therapeutic drug monitoring in pediatric patients and young adults with cancer. Ann Pharmacother. 2013;47:976-983. [CrossRef] [PubMed] [PMC free article]
- Hohmann C, Kang EM, Jancel T. Rifampin and Posaconazole Coadministration Leads to Decreased Serum Posaconazole Concentrations. Clinical Infectious Diseases. 2010;50:939-940. [CrossRef] [PubMed]
- Reusser P. Oral valganciclovir: a new option for treatment of cytomegalovirus infection and disease in immunocompromised hosts. Expert Opinion on Investigational Drugs. 2001 Sep 1;10(9):1745-53. [CrossRef] [PubMed]
- Kersun LS, Reilly AF, Coffin SE, Sullivan KE. Protecting pediatric oncology patients from influenza. Oncologist. 2013/01/31 ed. 2013;18(2):204-11. [CrossRef] [PubMed] [PMC free article]
|
|
| |
Cite this article as:
Dey M, Jain S, Shah I. Polymicrobial infection in immunocompromised host - How to manage?. Pediatr Oncall J. 2024;21: 134-137. doi: 10.7199/ped.oncall.2024.38
|