
Influenza A H1N1
Influenza A (H1N1) (referred to as "swine flu" early on) is a new influenza virus causing illness in people. This new virus was first detected in people in the United States in April 2009 with the 1st case in India being detected on May 16th, 2009. This virus is spreading from person-to-person worldwide, probably in much the same way that regular seasonal influenza viruses spread. On June 11, 2009, the World Health Organization (WHO) signaled that a pandemic of this novel H1N1 flu was underway, thus classifying it as Phase 6. This virus was originally referred to as “swine flu” because laboratory testing showed that many of the genes in this new virus were very similar to influenza viruses that normally occur in pigs (swine) in North America. But further study has shown that this new virus is very different from what normally circulates in North American pigs. It has two genes from flu viruses that normally circulate in pigs in Europe and Asia and bird (avian) genes and human genes. Scientists call this a "quadruple reassortant" virus.
Presentation
The symptoms of the novel H1N1 flu virus in people include fever, cough, sore throat, runny or stuffy nose, body aches, headache, chills, and fatigue, which are quite similar to those of seasonal flu. A significant number of people who have been infected with this virus also have reported diarrhea and vomiting.
When to suspect H1N1 influenza?
A child with a fever should be suspected to H1N1 influenza in the following circumstances:
- Within 7 days of close contact with a person who is a confirmed case of influenza A (H1N1) virus infection, or
- Within 7 days of travel to a community where there are one or more confirmed novel influenza A(H1N1) cases, or
- Resides in a community where there is one or more confirmed novel influenza cases.
Difference Between Swine Flu and Regular Seasonal Influenza
Swine flu is caused by a novel strain of the influenza virus called H1N1. This virus is spreading from person-to-person, probably in much the same way that regular seasonal influenza viruses spread. You will not be able to tell the difference between seasonal flu and influenza A (H1N1) without medical help. Typical symptoms to watch for are similar to seasonal viruses and include fever, cough, headache, body aches, sore throat, and runny nose. Like seasonal flu, H1N1 swine flu may cause a worsening of underlying chronic diseases. Only your medical practitioner and local health authority can confirm a case of influenza A (H1N1). If they suspect any symptoms they will send your blood sample, throat swab, and nasopharyngeal (nose to mouth) for testing to laboratories.
When Is H1N1 Influenza Dangerous?
In most patients, swine flu causes mild disease. Only in certain high-risk populations is the infection severe. Influenza A (H1N1) is a new virus and one to which most people have no or little immunity and, therefore, this virus could cause more infections than are seen with seasonal flu. Thus the overall vulnerability of the population can play a major role. For example, people with underlying chronic conditions, such as cardiovascular disease, hypertension, asthma, diabetes, rheumatoid arthritis, and several others, are more likely to experience severe or lethal infections. The prevalence of these conditions, combined with other factors such as nutritional status makes swine flu a dangerous infection for these patients to catch.
The following groups are at a higher risk for swine flu-related complications:
- Children less than 5 years old
- Persons aged 65 years or older
- Children and adolescents (less than 18 years) who are receiving long-term aspirin therapy and who might be at risk for experiencing Reye syndrome after influenza virus infection
- Pregnant women
- Adults and children who have chronic pulmonary, cardiovascular, hepatic, hematological, neurologic, neuromuscular, or metabolic disorders
- Adults and children who have immunosuppression (including immunosuppression caused by medications or by HIV)
- Residents of nursing homes and other chronic-care facilities.
Warning Signs
- Fast breathing or trouble breathing
- Bluish or gray skin color
- Not drinking enough fluids
- Severe or persistent vomiting
- Not waking up or not interacting
- Being so irritable that the child does not want to be held
- Flu-like symptoms improve but then return with fever and worse cough
Investigations
Though it is recommended that all patients with flu-like symptoms should be tested for H1N1 influenza, it may not be practically possible due to limited testing facilities. Besides, the infection is mild in most of the patients and is self-limiting. Thus, one may have to test only those patients who are at a high-risk group such as infants, patients with diabetes, heart disease, chronic illnesses, immunocompromised patients, and chronic lung disease.
The tests available at government testing centers are real-time RT-PCR, a viral culture, and tests that detect a rise in the antibodies against swine flu in the given blood sample. Apart from these, your local physician may perform a rapid dipstick test to diagnose Influenza A virus, and may then refer you to the government center to find out if you have specific Influenza A H1N1 or not.
Samples To Be Tested
- Throat Swab and Nasal/Nasopharyngeal Swab
- Blood for serological tests
- From an intubated patient: Lower respiratory aspirate and/or Blood for serological tests
Nasal swab: Insert the dry swab into the nostril and back to the nasopharynx. Leave in place for a few seconds. Slowly remove the swab while slightly rotating it. Use a different swab for the other nostril. Put the tip of the swab into a vial containing a viral transport medium, breaking the applicator’s stick.
Throat swab:
- Ask patient to open mouth and stick their tongue out
- Use tongue spatula to press the tongue downward to the floor of the mouth
- Use a sterile cotton swab to swab both of the tonsillar arches and the posterior nasopharynx, without touching the sides of the mouth
- Insert swab into the same transport tube containing nose swabs, break off the shaft and recap the tube firmly.
Storage of specimen prior to transport
Specimens should be stored at 4°C and transported within 48 hours. If the specimen cannot be transported in 48 hours it should be stored at -70 °C. Do not store in standard freezer or refrigerator. Sera may be stored at 4 °C for approximately one week, but thereafter should be frozen at -20°C. Specimens collected for influenza virus isolation should not be stored or shipped in dry ice (solid carbon dioxide). Carbon dioxide can rapidly inactivate influenza viruses if it gains access to the specimens through imperfect seals. is collected from the anterior turbinate.
Treatment
Treatment is largely supportive and consists of bed rest, increased fluid consumption, cough suppressants, and antipyretics, and analgesics (eg. Acetaminophen, non-steroidal anti-inflammatory drugs) for fever and myalgias. Aspirin should be avoided in pediatric patients to avoid Reye’s syndrome. Severe cases may require intravenous hydration and other supportive measures. Antiviral agents may also be considered for treatment or prophylaxis. CDC recommends the use of oseltamivir or zanamivir for the treatment and/or prevention of infection with the swine flu virus. Antiviral drugs may reduce the symptoms and duration of illness, just as they do for seasonal influenza. They also may contribute to preventing severe disease and death.
Figure: Algorithm to manage H1N1 influenza
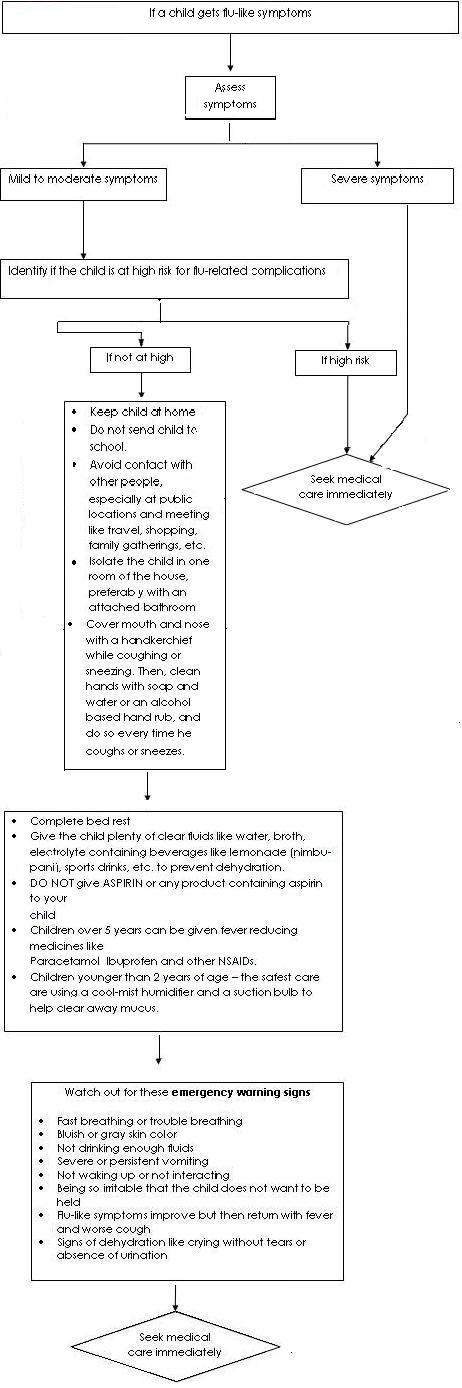
Table 1. Antiviral medication dosing recommendations for treatment or chemoprophylaxis of novel influenza A (H1N1) infection. (Table extracted from IDSA guidelines for seasonal influenza.)
| Agent, group |
Treatment |
Chemoprophylaxis |
| Oseltamivir |
| Adults |
75-mg capsule twice per day for 5 days |
75-mg capsule once per day |
| Children >_ 12 months |
15 kg or less | 60 mg per day divided into 2 doses | 30 mg once per day |
16-23 kg | 90 mg per day divided into 2 doses | 45 mg once per day |
| 24-40 kg | 120 mg per day divided into 2 doses | 60 mg once per day |
>40 kg | 150 mg per day divided into 2 doses | 75 mg once per day |
| Zanamivir |
| Adults | Two 5-mg inhalations (10 mg total) twice per day | Two 5-mg inhalations (10 mg total) once per day |
| Children | Two 5-mg inhalations (10 mg total) twice per day (age, 7 years or older) | Two 5-mg inhalations (10 mg total) once per day (age, 5 years or older) |
Table 2. Dosing recommendations for antiviral treatment of children younger than 1 year using oseltamivir.
| Age |
Recommended treatment dose for 5 days |
| <3 months | 12 mg twice daily |
| 3-5 months | 20 mg twice daily |
| 6-11 months | 25 mg twice daily |
Isolation
In the hospital:
- Place patients in a single-patient room with the door kept closed. Isolation facility needs to have negative pressure, air control (10-12 air changes per hour), double door entry, and dedicated staff. Air can be exhausted directly outside or can be recirculated after filtration by a high-efficiency particulate air (HEPA) filter.
- If a dedicated isolation room is not available, then patients can be kept in a well-ventilated isolation ward with beds kept (at least) one meter apart.
- Aerosol-generating procedures such as endotracheal intubation, nebulized medication administration, induction and aspiration of sputum or other respiratory secretions, airway suction, chest physiotherapy, and positive pressure ventilation should be performed by the treating physician/nurse wearing a full complement of PPE with N95 respirator on.
- Hospitals with centralized air conditioning are not allowed by the Government to treat swine flu cases as the centralized AC may help in the spread of infection within the hospital.
- Until further evidence is available, infection control precautions should continue in an adult patient for 7 days after resolution of symptoms and 14 days after resolution of symptoms for children younger than 12 years because of a longer period of viral shedding expected in children. If the patient insists on returning home, after the resolution of fever, it may be considered, provided the patient and household members follow recommended infection control measures, and the cases could be monitored by the health workers in the community.
At home:
- Infected person should stay home for seven days; preferably isolate himself/herself in a well-ventilated room. Avoid common areas frequented by other family members of the family.
- If the living space is small and more than one person need to sleep in a room, ensure that the head end of the patient and others sleeping in that room are in the opposite direction
- Infected person should wear a mask all the time.
Prevention and Prophylaxis for Health Care Workers
Health care personnel who may come in contact with patients suffering from H1N1 influenza should take precautions when dealing with suspected cases. They should wear proper masks for the prevention of transmission of infection. After a thorough hand wash, wear the gown, followed by goggles, shoe cover, head cover, face mask, and finally gloves. Similarly, remove the gown followed by gloves. Wash hands thoroughly and then remove the head cover, face mask (by grasping elastic behind ears - do not touch the front of the mask) and goggles and again wash hands thoroughly. After leaving the room, again wash hands thoroughly.
Health care personnel at medium-high risk: These persons should wear complete protective equipment including masks (N-95), gloves, protective eyewear (goggles), hair covers, boot or shoe covers, and gown or apron. The personnel include
- Medical and nursing staff involved in clinical examinations at the airport and quarantine center
- Medical personnel involved in sample collection
- Rapid Response Team while transporting or attending a suspect case in the ambulance
- Health staff involved in managing a suspect case at the health facility
- Staff handling the dead body of a suspect/probable/confirmed case
Health care personnel at low-medium risk: These persons will only need a three-layered surgical mask. They include
- Paramedical staff involved in a public health screening at the airports.
- Immigration and other ground staff at the airport
- Passengers in the same row, three rows in front and three layers behind a suspect case
- Health workers involved in surveillance
- Rapid Response Team during supervisory field operations
- Security personnel involved in quarantine, social distancing measures, law and order maintenance
- Personnel providing essential services
- Close household contacts of a suspect/probable/confirmed cases
Precautions in OPD
While dealing with patients with flu-like symptoms, the doctor must carry out the following safety precautions:
- Clean hands before and after every patient interaction, preferably with alcohol-based disinfectants.
- Wear a disposable facemask or respirator.
- Segregate patients with flu-like symptoms in a separate waiting area; those patients who can tolerate facemasks should be asked to wear them.
- While collecting throat/nasal swabs - wear a facemask or respirator, gloves, and protective eye equipment.
- Keep all surfaces in your OPD clean
PROPHYLAXIS
Ideally, all health care personnel coming in contact with suspected, probable or confirmed cases of H1N1 influenza should receive post-exposure prophylaxis. Oseltamivir is a drug recommended for the treatment of swine flu. It can be given as post-exposure prophylaxis to contacts of H1N1 influenza patients. However, doctors may get repeated exposure to the H1N1 influenza virus and repeated courses of prophylaxis may not be useful and may have side effects. Prophylaxis should be provided until 10 days after the last exposure (maximum period of 6 weeks).
Surgical Masks and Respirators
A facemask or a respirator needs to be used in one of the following conditions only:
- For a person who is at increased risk of severe illness from influenza, and if there is a new outbreak of swine flu in the community in a crowded environment, a facemask or a respirator may be considered only if the crowded setting is unavoidable.
- For a person who is at increased risk of severe illness from influenza, and if he/she is a caregiver to a person with influenza-like illness, a facemask or respirator is recommended only if being the caregiver is unavoidable. If you are caring for a sick person, you can wear a mask when you are in close contact with the ill person and dispose of it immediately after contact, and clean your hands thoroughly afterward.
- For a person who is at increased risk of severe illness from influenza, and if there is exposure in an occupational setting (but not health care) when there is an outbreak of swine flu in the community, use of a facemask or respirator may be recommended under certain conditions.
- For persons who may or may not be at increased risk of severe illness from influenza, but who are exposed in an occupational setting, providing care to persons known or suspected to have swine flu, respirators are recommended.
Using a mask correctly in all situations is essential. Incorrect use increases the chance of spreading infection. A face mask or a respirator is not necessary for persons who are not included in the above categories.
N95 RESPIRATOR
There are important differences between facemasks and respirators. Facemasks do not seal tightly to the face and are used to block large droplets from coming into contact with the wearer’s mouth or nose. Most respirators (e.g. N95) are designed to seal tightly to the wearer’s face and filter out very small particles that can be breathed in by the user. For both facemasks and respirators, however, limited data is available on their effectiveness in preventing transmission of H1N1 (or seasonal influenza) in various settings. However, the use of a facemask or respirator is likely to be of most benefit if used as early as possible when exposed to an ill person and when the facemask or respirator is used consistently. The use of N95 respirators or facemasks generally is not recommended for workers in non-healthcare occupational settings for general work activities.
An N95 respirator in addition to blocking splashes, sprays, and large droplets is also designed to prevent the wearer from breathing in very small particles that may be in the air. To work as expected, an N95 respirator requires a proper fit to your face. Generally, to check for proper fit, you should put on your respirator and adjust the straps so that the respirator fits tight but comfortably to your face. For information on proper fit, refer to the manufacturer’s instructions.
The 'N95' designation means that when subjected to careful testing, the respirator blocks at least 95% of very small test particles. If properly fitted, the filtration capabilities of N95 respirators exceed those of face masks. However, even a properly fitted N95 respirator does not eliminate the risk of illness. N95 respirators are not designed for children or people with facial hair. Because a proper fit cannot be achieved on children and people with facial hair, the N95 respirator may not provide full protection. People with chronic respiratory, cardiac, or other medical conditions that make it harder to breathe should check with their healthcare provider before using an N95 respirator because the N95 respirator can require more effort to breathe. Some models have exhalation valves that can make breathing out easier and help reduce heat build-up.
N95 respirators are labeled as "single-use", disposable devices. If your respirator is damaged or soiled, or if breathing becomes difficult, you should remove the respirator, discard it properly, and replace it with a new one. To safely discard your N95 respirator, place it in a plastic bag, and put it in the trash. Wash your hands after handling the used respirator.